

By Michael Barker, PA-C and Daniel Parkinson, M.D.
Note to readers:
This blog post is very data driven. To help with the flow of the blog post, the studies referenced throughout are cited, footnoted, and expanded upon in the notes and resources section following our main essay. We strongly encourage all readers to read the notes and resources section to be better informed.
Recently, a local operating room saw a small spike in post-operative infections. This caused a beehive of activity among the administration as they quickly looked for ways to bring the infection rate down. They formed a committee of nurses, a few doctors, orderlies, and non-medical staff and asked them to brain storm and throw ideas out as to what caused this spike and suggestions as to how to fix the rise in infections. Believe it or not, many of those ideas and suggestions were taken seriously. Is there a problem with this method? Yes.
- The doctors pointed out that it was never investigated to see if the bump in infections was statistically significant. Was this bump within the normal standard of deviation?
- Evidence base medicine was not used to address the problems.
When people approach such things frantically and with little information, policies are put into place that may or may not correct the problem being addressed. Sure, administration feels great, but the rest of us are just shaking our heads and wondering why we have to do all the extra work that has no science to support it. Already some of these policies are no longer enforced. Why? Because they are tedious and probably don’t help. Some of these policies will be in place for years until at one point everyone starts asking, “So why are we doing such and such?” The answer will be, “We don’t know.”
So what does this have to do with lesbian/gay/bisexual/transgender/queer (LGBTQ) suicides in the LDS community?
When we are talking about LBTQ suicides, we need to make sure we are working with the best empirical evidence available. Otherwise state and federal policies will be put in place that may offer no help. Everyone will feel great about themselves—except our LGBTQ youth. We need to make sure the evidence presented is being interpreted correctly. Otherwise poor government policies will be put in place that may offer no benefit or might even exacerbate the problem. We will then be asking the same questions, “Why are we doing this?”
This blog post will look at five things and our attempt to look at these five things may be a bit audacious, but here we go:
- What direct empirical evidence is available regarding LGBTQ suicides?
- What is the indirect evidence?
- What is the anecdotal evidence?
- What conclusions can we draw taking into account the limitations of empirical, inferred, and anecdotal evidence?
- What preventive measures should be implemented while we are waiting for more definitive empirical evidence?
What is the direct empirical evidence?
- National studies show that LGBTQ teens are at a much higher risk of suicide attempts.1
- Family Acceptance Project (FAP) has done some excellent research showing that there is an exponential risk of suicide for LGBTQ teens who come from families that show rejecting behaviors. They even studied what those rejecting behaviors are, and anyone familiar with the Mormon community would recognize those rejecting behaviors as being very common in our communities. Rejecting behaviors by parents are even reinforced by local church leaders and Mormon culture (refer to FAP info). It is also important to note that the risk of suicide remains higher well into adulthood. These youth also have exponentially higher rates of drug/alcohol use, depression, and HIV infection compared to youth raised in homes that don’t show these rejecting behaviors.2
- Schools with explicit anti-homophobia interventions such as gay-straight alliances (GSAs) may reduce the odds of suicidal thoughts and attempts among LGBTQ students.3
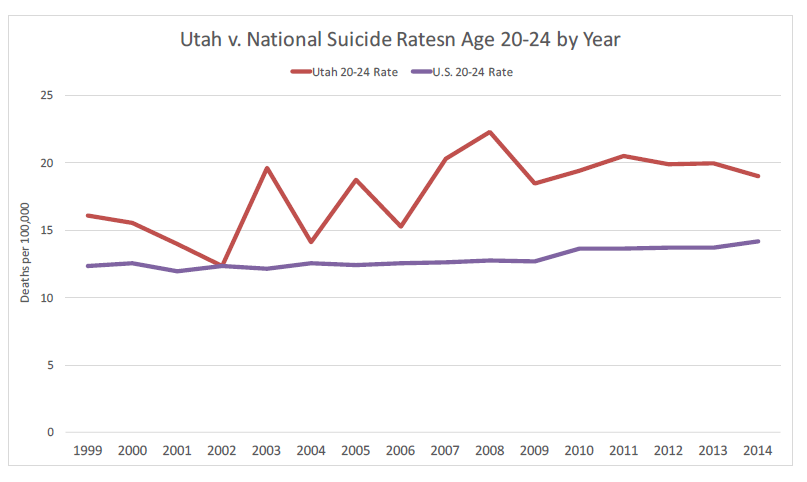
- Suicide is the number one cause of death of all Utah youth; this is not the case nationally. More alarming, the teen suicide rate in Utah has doubled since 2011.4
- Teen suicide is lower when there is an LGBTQ supportive environment.5 Unfortunately, isolation (a risk factor for suicide) is more prevalent among LGBTQ people. For example, one study shows that lesbian, gay and bisexual Australians are twice as likely as heterosexual Australians to have no contact with family or no family to rely on for serious problems (11.8% v. 5.9%).6
There is a clear body of research showing that there is an elevated risk of suicide among LGBTQ teens nationally. There is also a clear body of research showing what the major risk factors are for suicide and other poor outcomes for LGBTQ youth. There is no reason to believe that the LDS community is immune to this. Based on this alone, we do need to consider that we have a suicide problem in our community. Analysis of the data suggests that the problem is worse in LDS communities than the national average. The youth suicide rate in Utah is the first statistic that implies this. Although the suicide rate is elevated throughout the intermountain west,7 no other states have seen the doubling in the teen suicides that Utah has had in the past 4 years. Why is youth suicide in Utah so much higher than the national average? Since LGBTQ issues may be a large factor impacting teen suicides, it would be irresponsible not to address these issues locally, especially when the suicide problem is so acute in Utah, where the highest concentration of Mormons live. Meanwhile, studies have shown us the risk factors for suicide, but protective factors have not been studied as extensively or rigorously as risk factors.7a
What is the indirect evidence?
- Studies show that in cities/regions where homosexuality is tolerated, mental health outcomes for LGBTQ are the same as non-LGBTQ people. We can infer from this that an elevated risk of suicide would correlate with the elevated risk of mental illness that is prevalent among LGBT people living in communities that are hostile to LGBTQ.8 In general, Utah communities are hostile to LGBTQ people.
- Another statistic that goes hand in hand with suicide is youth homelessness; the two are highly correlated. National studies show an exponentially higher risk of homelessness among LGBTQ teens. Providers and outreach workers in Utah have noticed that this also applies to Utah, and they have noted a high rate of LGBTQ teens from LDS families among the homeless teens they serve.8a
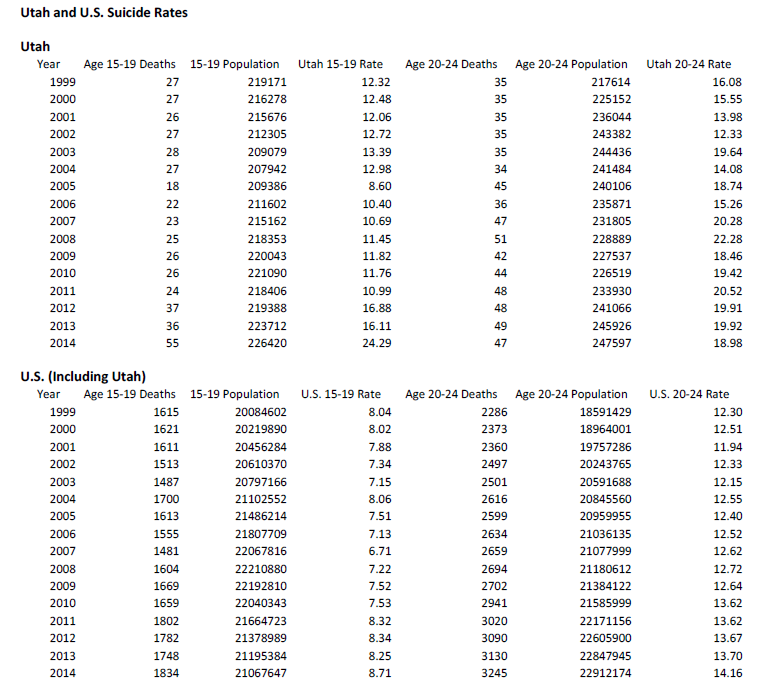
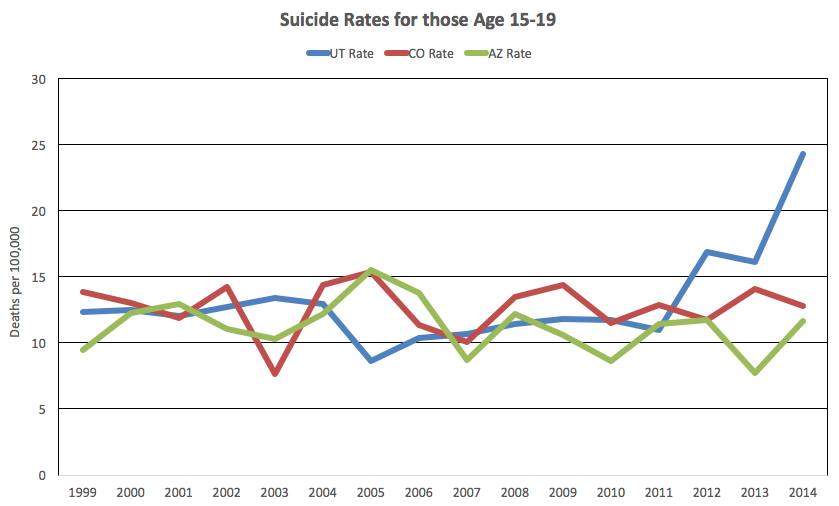
- As noted above, data from the CDC shows that suicides in the 15-19 age range in Utah have doubled since 2011. The graphs and table shown below don’t include 2015 but preliminary indications are that 2015 data for age 15-19 are similar to 2014 data. While Utah had a doubling of suicides among teens, the rest of the country did not see a substantial increase in their suicide rate. Suicide has become the number one cause of death in this age group in Utah. Correlation doesn’t prove causation, but it is important to look at correlating factors to determine which of these factors might explain causation. The time frame for this doubling of teen suicides does correspond to an increased focus in the media on LGBTQ issues, especially in Utah as the debate on same-sex marriage played out. That clearly led to a backlash, including frequent church statements criticizing same-sex marriage or criticizing the LGBTQ community. These statements have reinforced conflicts within congregations and within families over the issue and has unleashed an increase of demonstrated homophobia and anti-LGBTQ feelings within families. It can easily be inferred that this chain of events exacerbated family rejection of vulnerable LGBTQ teens, thereby increasing their risk of suicide attempts as shown by the Family Acceptance Project (see footnote 2).
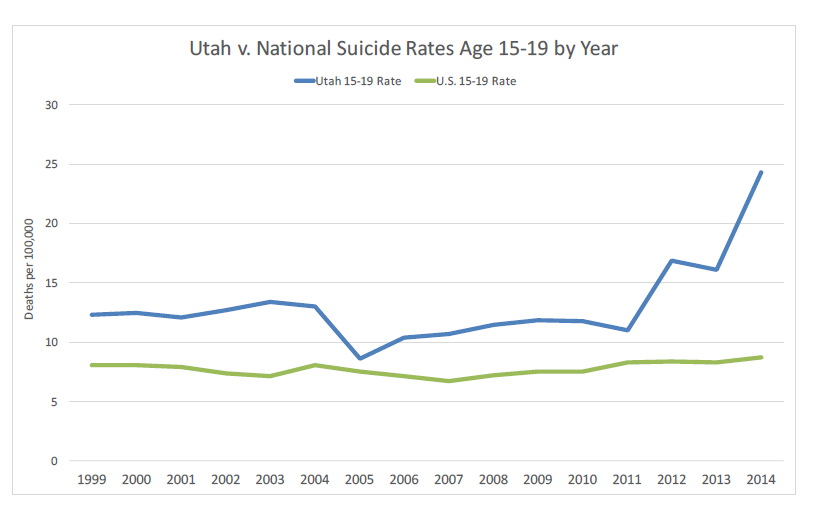
The above data is publicly available from the Centers for Disease Control and Prevention at http://www.cdc.gov/injury/wisqars/ Chart and graphs by Dr. Phillip Rodgers, Ph.D. Note: While Utah suicide rates are higher than the National average, they are generally in line with other Rocky Mountain States (although only Utah has seen this doubling of suicides among teens over the past 4 years). Note: Suicide is a complex behavior that is influenced by multiple factors that vary across individuals. (please see footnote 4 for more graphs)
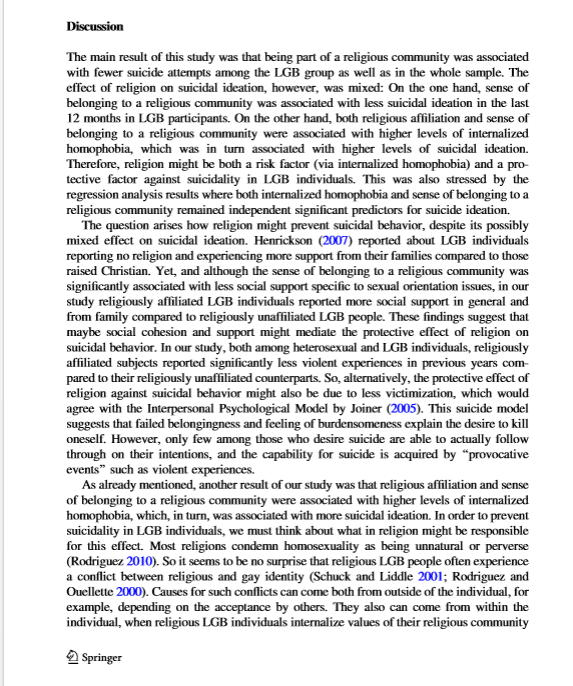
- A study of Mormon men in Utah shows that leaving the Church puts one at a much higher risk of suicide. It appears that LGBTQ people leave the church or are kicked out at very high rates. Can we, from these studies, infer that these LGBTQ men are among those who have a substantially higher risk of suicide when they lose the protection that membership in a religion provides against suicide risk?9 (see also footnote 5) If so, then bishops, stake presidents, and family members have reason to worry when an LGBTQ person stops attending Church. In general, the effect of religion on suicidal ideation is mixed. However a recent study suggests that religion may be protective against suicide attempts, even when LGBTQ people have “internalized homophobia.” However, this same study shows once again that maturing in a religion increases the risk of suicide among those who leave.10 Once again, it can be inferred that LGBTQ people are placed at higher risk because of their tendency to feel unwelcome in their religious communities and end up losing the protection of religious involvement.
These studies, observations, and data don’t directly answer our questions about LGBTQ suicides, but they are a smoking gun. They help us to infer reasonable conclusions beyond what the studies directly show. In the above cases, the inferred conclusions can be very compelling, and give us valid concerns especially when there is such a broad range of evidence that demonstrate a problem in our community. However, direct research will still be needed to clarify any factors that might have been misleading.
What is the anecdotal evidence?
- Anybody who knows a substantial number of LGBTQ people from LDS backgrounds will be astounded by how many have had suicidal attempts. (Dr. Parkinson has personally observed it among those that he knows). Those who are in a particular position of outreach such as the leadership of Affirmation, Wendy and Thomas Montgomery, or Carol Lynn Pearson are also very overwhelmed by the consistent pattern of suicidal ideation and suicidal attempts and suicides among LGBTQ people from Mormon backgrounds particularly youth and young adults.
- Clinicians who have worked with teens in Utah including clinicians from LDS Family Services have noticed the high rate of despair and suicidal thoughts among LGBTQ teens (as well as adults). Several clinicians have discussed this trend in their practices in media interviews including Hollie Hancock and Lisa Tensmeyer Hanson.
- Polling of USGA (a support organization for LGBTQ BYU students) showed a very high rate of suicide attempts among its members as they have described here and here. Informal polling of LGBTQ youth on a Facebook group for LDS LGBTQ youth has also revealed the ubiquitous nature of suicidal thoughts among our LGBTQ Mormon youth
Anecdotal evidence is not research based, and therefore is also much more subject to bias due to sample size, prejudice or any number of other factors. However, when the anecdotal evidence becomes massive (as it has to those of us who work directly with LGBTQ Mormons around this issue) then we must pay attention to it. We don’t always need a scientific study to inform us when our collective experience is so vast. For example, if we assert that most people from the South have a southern accent, and a lot of people who live in the South agree with us, then it is reasonable working hypothesis until the day that somebody does a study to determine what percentage of Southerners actually do speak with a southern accent. If we interview 100 gay people and notice that the vast majority of them have seriously considered suicide, and that their Mormon experience exacerbated their despair and suicidal thoughts, and then we speak with other clinicians who have observed the same, then it is worth taking seriously. Perhaps a better analogy is this: If Syrian refugees arrive on the islands of Greece and announce that many refugees are drowning and we can physically see bodies washing up on shore, we can’t wait for exact numbers before we start to think about prevention. We also need to ask those refugees what led to the drownings and pay attention to their accounts.
What conclusions can we draw?
When we put this data together we can’t know exactly how many suicides there are among Mormon youth and how many of these are related to LGBTQ issues.12 However, we have some extremely compelling evidence that allows us to conclude that there is a significant problem. The direct empirical evidence alone is enough to merit a public health response.
The indirect evidence is also very compelling, because there are such close correlations between suicide and mental illness/mood disorders, as well as homelessness in general, and LGBTQ people have a higher prevalence of these, at least in homophobic communities. This truly suggests that LGBTQ suicides are higher in these communities.
In the case of LDS youth suicides, we are forced to pay attention to indirect evidence and anecdotal evidence because it is so difficult to gather empirical evidence about any suicide cohort because of the stigma associated with it, as well as the intense grief experienced by these families. Some families are in denial that their family member is LGBTQ. Furthermore, those youth at highest risk are often the same youth who will hide their sexual orientation, so the family may not even be aware. As one Provo police officer said, “They don’t leave a note saying they died by suicide because they are gay.” It is often difficult to tell if an accidental death is actually a suicide, so those will be missed by any inquiry. Investigating whether sexual orientation is a factor in suicide is clearly complicated, and state agencies in Utah (and other states) have been reluctant to do so.
Normally we should be reluctant to make decisions based on anecdotal evidence alone. However, when the anecdotal evidence is highly compelling and lives are at stake as can happen in any public health crisis, it is critical to be very proactive. Let’s not forget the government’s response to HIV. Stigma and denial led to a needless delay in finding causes, treatments, and cures. How many thousands of lives could have been saved if they would have responded immediately as they should have? Another illustrative example from HIV research was the ethical problems of withholding treatment until the cures can be proven. Physicians finally decided to work with activists and to allow compassionate treatment with unproven medications because it was the only chance these patients had to possibly survive. The normal approach of waiting for definitive empirical evidence proved to be unethical in this situation.
Presently, a public health action is even more compelling because we have identified preventive measures that are low cost, low risk, and have already been shown to be effective. Currently the problem is not a lack of evidence, but a lack of will. We have sufficient direct evidence that is strengthened by indirect evidence, and reinforced by anecdotal evidence. The case is extremely strong. Denial and misinformation are our biggest barriers to implementing effective public health measures that have already been recommended by experts.
In the end, determining if LGBTQ people are more likely to die by suicide is difficult to determine empirically due to contradictory studies, small sample sizes, and difficulty obtaining data about deceased individuals. Presently, one cannot conclusively determine that LGBTQ youth are more likely to die from suicide. This does not diminish our responsibility to take measures to decrease their suicides by decreasing their attempts—and that is within our reach.13It is also within our reach to decrease the depression, despair and isolation that afflict our LDS LGBTQ youth.
Homelessness, despair, depression, suicide attempts, social isolation, bullying—these all call out for an active response from the Church, the State, and our communities. There is a wealth of direct evidence showing that these problems have a huge impact on LGBTQ people including LGBTQ Mormons. Those issues on their own and the human suffering that accompanies them also warrant a public health response, even before suicide is taken into account. We shouldn’t need to prove the suicides in order to address these issues that so greatly impact the lives of so many among us.
Discussion: What drives the despair?
- Fear of isolation
- Fear of ostracism, fear of being a social pariah
- Fear of disapproval, fear of shunning, fear of assault or bullying
- Fear of rejection by family or community, fear of homelessness
Depression and mood disorders play a role in many if not most suicide deaths or attempts. But what can we look at from a community standpoint? What are the factors that put people at risk and then put some of them over the edge?
Neuroscientist Michael Ferguson pointed out in a recent podcast interview that “as social beings when you’re shunned or you’re excommunicated or you’re rejected from your primary community of attachments, your body experiences that like you’re preparing to die.”13a Humans are social creatures, and historically, surviving without our most important social connections was impossible. Being cast out was literally deadly. To a social animal such as a human, there are few things worse than ostracism.
Look at it through the eyes of an LGBTQ teen. They know they are an LGBTQ person. They often fear losing their family if their family finds out. The church reinforces that for them by making them fear that they won’t be part of the eternal family. An entire future is mapped out for them that they know they can’t fit into. They face bullying at school and at church, and they can’t get any support from their parents around the issue because they are too frightened to tell their parents. Meanwhile their parents reinforce this at home by making homophobic comments which cement the child’s concerns that they risk losing their family if they come out, and that they might also lose their shelter and education by being kicked to the streets. Meanwhile, hostile messages surround them at church, school, and home. Like every teen, they start to develop feelings and dreams of love and companionship, but then they get the message that their desires are evil, and that in order to be accepted they have to follow a path that feels impossible for them. Most LGBTQ Mormons have this experience to varying extents. Many of them work their way through it and survive. However, many have other problems, such as depression, or poor family structures. The despair often leads them to risk-taking behaviors and substance abuse. These factors stack up and multiply their odds of having a suicide attempt or other dangerous behavior such as drug use or unprotected sex.
In the past there were very clear messages that suicide was the best option for them. Even today some local leaders advise youth that they would be better off having a shortened, “pure” life than a full life in a same sex relationship (hopefully that is decreasing, but unfortunately it still happens).13b There is also the implied message that still reaches a large number of these youth—that the only chance they have of being with their families in heaven is if they kill themselves. They try to uproot this ‘evil’ within them, but they are doomed to fail. They don’t see a future worth living, and they don’t want to sin and lose their chance to be with their families in heaven. So they resolve to kill themselves before they commit any serious sin that would jeopardize their eternal life.
We have all heard in church of the father who would rather have his son come back in a casket than have him come back without his honor. This belief still permeates our culture. There are plenty of sons and daughters who have chosen the casket believing that this was what their parents would prefer.
Since the majority of LDS families are indeed strong families whose homes are full of love, members of these families assume that if their children were feeling conflicted, they would know about it. They can’t imagine that their child would be afraid to disclose feelings of despair, isolation or thoughts of self harm. This is a prevalent assumption of parents, especially those who focus so much time and energy on their families. But these loving parents are sending rejecting messages long before they realize that their child might be LGBTQ.
Do dinner table politics and conversations denote a negative/sad connotation of LGBT people or seek to restrict inclusion in any way? Are missions and temple marriages held up as the ideal life path; the one that would make the parents the most proud? If a child’s biggest desire in life is to make their parents proud, what ideal is being upheld? Having a loving family isn’t enough. Parents need to actually sit down with their kids throughout their youth and specifically say “We will love and be proud of you if you marry a boy or a girl or don’t marry at all. Though missions are important, we know that isn’t always possible for everyone and that’s okay too. We will stand up for you and your choices. We will help you the best we know how, no matter what; even if we don’t understand at first. If at some point your life goals feel different than what we currently know about you, we want to discuss that together and understand what your life direction means to you personally. Not being exactly like us should never cause you to fear us being disappointed in you.” Until that conversation is being had in the homes of every LDS family, we will continue to see LGBTQ people suffer in isolation.–Lori Burkman
Any single suicide is multifactorial. Being a LGBTQ person in a homophobic society is certainly a risk factor. Having a rejecting family is a huge risk factor. Ostracism and bullying are risk factors. Depression and other mood disorders are huge risk factors. Poor coping skills, social isolation, marginalization and stigma are all risk factors. Some of these risk factors are direct outcomes of the way these LGBTQ teens are treated by their family and by their community. Others factors, such as an inherited mood disorder or impulsivity are certainly exacerbated by any rejection or ostracism. Because of the homophobic climate in our communities, LGBTQ Mormons are a vulnerable population at baseline. Even the most healthy LGBTQ teens suffer substantially. If a child has a genetic predisposition for major depression or another mood disorder, then you combine that with those problems that frequently impact LGBTQ people—family rejection, bullying, ostracism, substance abuse, etc., you end up with a combination that leads to intense isolation and despair, which then can fuel a tragic outcome.
The political system in Utah is reflection of the Mormon church and the Mormon community. It is very clear that the Mormon majority in the Utah legislature are very responsive to what the church leaders support, and the church regularly influences legislation openly, such as when they supported a compromise that allowed passage of a statewide anti-discrimination bill that gave substantial exemptions based on religion. Meanwhile, the state legislature has been very hostile to LGBT youth. There is a ban on discussing any LGBTQ issue in public schools (see footnote 11). This makes it very difficult for schools to adopt measures that will help combat bullying and create a safe learning environment for LGBTQ youth. That would change in an instant if the church threw their support behind measures to help our vulnerable teens. Marian Edmonds-Allen, Utah’s leading advocate for LGBTQ youth, laments the situation in our schools:
“Compounding the risks in Utah is an environment that restricts not only the gathering of data but also the sharing of lifesaving information. State school board guidelines that prohibit “the advocacy of homosexuality” are directly contributing to risk of suicide for youth, both LGBT and straight. Gay-straight alliances, which have been shown to provide a 50 percent reduction in suicide risk for males, both GBT and straight, are becoming even more rare in Utah. New GSAs are routinely refused because the word “gay” is in the title, and many GSAs in the state have been replaced by “Hope Squads,” ostensibly to help prevent suicide, but which do not include any reference or supports for LGBT students.”14
As the law now stands in Utah, school counselors are not allowed to address relevant issues with LGBT youth who report suicidal thoughts, nor are they allowed to give parents helpful information/resources or even explain the problem when their child is feeling rejected due to their sexual orientation or gender identity. One can see how this puts undue stress on LGBTQ teenagers who are left with nowhere to turn for support.15
Even more alarming is the glaring lack of resources for homeless teens. Like the rest of the nation, a disproportionate number of homeless teens are LGBTQ. Whether gay or straight, their lives in the streets and canyons of Utah are bleak. Until one year ago there was not a single shelter bed available to these youth which number up to 1000 at any point in time. Even now there is only one shelter that can house 16 youth; a mere drop in the bucket. Laws that supposedly protect parental rights have made it impossible for any law-abiding citizen to offer shelter to any of these children, meaning that to survive these youth often had to turn to prostitution or exploitation by adults. Drugs become the only escape from their bleak existence but further increase their vulnerability and dependence on their exploiters.
So while Utah is making headlines because of their innovative, compassionate and effective approach to adult homelessness, 1000 youth are in a state of total abandonment. Almost half of these are LGBTQ. Over half of these come from LDS homes. They have been abandoned by their families. They have been abandoned by their wards and bishops. They have been abandoned by the state. They may as well be living in Calcutta. The only thing outreach workers could do for them is help them find a sleeping bag and maybe a coat and send them on their way. This is happening a few blocks away from the Church Office Building and the Capitol. If the church and the government can cooperate to clean up downtown Salt Lake City by building a beautiful shopping center, can’t they set ideology aside long enough to rescue these children?
But like in our schools, there is no discussion allowed around LGBTQ issues. Parents are not taught in church that they must love their LGBTQ children nor how to protect them.16 Youth are not taught that they should include their LGBTQ peers in activities. Youth leaders are not taught to watch for bullying. Bishops are not taught how to respond to LGBTQ teens who come to them in despair, with no hope for the future. There are no church-fostered support groups.
The only message that our LGBTQ youth hear at church is how godless and eternally destructive gay people are. They are given messages that God disapproves of who they innately are. They are taught that the only thing worth living for is temple marriage, which they know they can’t attain. There is never a single message given in church that is directed to their needs in a way that offers hope; the closest they get is a recommendation to stoically live out their days in celibacy and solitude as they watch everyone around them pursue relationships and families of their own. They are then mistreated by their peers and ostracized for seeming gay. This dynamic persists in their homes. They feel cut off from their peers at church and at school. They feel cut off and rejected by their families. Meanwhile, their families have no idea how much damage they are causing with their rejecting stances. They believe they are preserving their family by being harsh against ‘sinful LGBTQ behavior’. And if they try to advocate for their LGBTQ child, they too will often experience ostracism from the same wards, and that becomes a disincentive to a healthy, compassionate response. Then as the child gets older and feels increasingly alienated from their religious community and its teachings, these youth see no reason to obey Mormon rules and are more likely to explore drugs, alcohol, or sexual behavior at an early age. They then get labeled rebellious, which exacerbates their conflicts at home and at church. It is a perfect storm. The situation deteriorates, especially when you add in any other problems such as loss, trauma, depression, attention deficit disorder, or learning problems.
All of this situation is the background and is a constant in our LDS community. It is enough to warrant a serious response. However, all of these stressors to our youth become exacerbated any time there is a declaration or policy speaking out against same-sex marriage (or homosexuality, or participation in boy scouts…). These statements are difficult for these youth to absorb. There is substantial pain/despair that comes from just hearing the text. But that is only the beginning. These public statements and letters that are read within their wards serve to reinforce all of the rejecting behaviors that they face from their families and communities. They embolden people to make harsh homophobic comments from the pulpit and in Sunday School classes. Parents, and relatives increase their expressions of disgust and dismay about homosexuality in the home or on Facebook. The increased attention that comes with these declarations is universally negative for these teens. Their isolation increases right when they are most vulnerable. There is occasionally a footnote included in these church statements that we need to be civil, but there is never a reminder that there are vulnerable teens in our midst who will absorb these hurtful comments that are unleashed. Instead of being a refuge, church feels like a war zone to these youth, a place of misery, of despair. Is that what our church should feel like for anybody?
Discussion: Did the exclusion policy impact suicide numbers?
It is important to remember that there was already a major problem with suicide among LGBTQ Mormons that is a long-standing issue as well as depression, homelessness, suicide attempts, and despair, long before the recent policy was revealed.
—Bad question: Were there really 34 suicides of LGBTQ people since policy announcement?
—Good question: Is further rejection and homophobia in our communities increasing depression and despair and consequently intensifying the conditions that contribute to the elevated suicide rate in our community?
As stated above, people in positions of outreach such as the Affirmation leadership and the Mama Dragon leadership found themselves dealing with LGBTQ people in distress, and often found themselves spending late nights consoling people who were struggling with suicidal feelings. Due to her high visibility in the media, Wendy Montgomery had already had a constant stream of LDS people reaching out to her around this issue to tell her their stories, and seek support and resources. This had been going on for the past few years and had basically turned into a full time job for her. However, after the policy was revealed in November, she started getting more and more reports from LDS people who were describing that an LGBTQ family member had died from suicide. She eventually added up these informal reports and found that there were 32 deaths from suicide reported to her between Nov. 6, 2015 and Jan.17, 2016 (the number rose to 34 later that month). She ended up reporting those numbers to John Gustav-Wrathall, the President of Affirmation who mentioned them in a public address that he gave on Jan. 17, 2016, which eventually led to a lot of media attention and debate.
The data reported by Wendy Montgomery seem confusing because, while she did get a high number of reports of suicide since November 6, it is hard to square these numbers with the State of Utah who reports that there were only 10 suicides in Utah in November and December of 2015 in the 14-20 age range. This discrepancy was reported in the Salt Lake Tribune (see footnote 11). Unfortunately the article did not give a deeper analysis of discrepancy. We have to be aware that the State will always underestimate actual suicides for several reasons, especially because it will not consider an overdose or an accident a suicide, even though overdoses and accidents are both very common ways of attempting/completing suicide. The Utah numbers also did not include out-of-state numbers, numbers outside of the 14-20 age range and numbers from January. Therefore the number of suicides of youth and young adults is clearly higher than 10. Since the reports sent to Wendy Montgomery weren’t solicited, precise statistical information was not obtained. She has stated that the reports were not always precise and did not always state when the suicide took place, so it is possible that some of them took place prior to the policy change. It is likely that these factors explain the discrepancy.
It is pretty compelling that so many families reached out to the her in the first place. She did not solicit this information. Wendy Montgomery and the Mama Dragons have been very high profile in the media lately and have put themselves out there as a resource, so it is not surprising that people reach out to them in times of need. They had been getting reports of suicide since their formation two years ago. However, this influx of reports justifiably raised her concerns. This was not a statistical analysis, and she was unable to release the exact details due to privacy. However, she and others felt compelled to respond to this influx of reports, as they should have.
There are those who think that these numbers were invented for the press. We don’t have any way to convince dubious people of the integrity of these amazing individuals aside from vouching personal friendships and years of close collaboration with them. Even though they clearly disagree with the church on the policy, that would not be their modus operandi to invent a narrative like that. In fact, they have had experiences with false suicide reports and have seen the damage those can have to the credibility of the movement.
We know that LGBTQ Mormons are a vulnerable group. Those who work with them as activists and clinicians have noted the despair among LGBTQ Mormons since the policy announcement that is unrivaled by anything they remember from past traumas (Prop 8, Boyd K Packers’ famous quote, etc). We have also noted an upswing in overt hostility toward LGBTQ people in our wards, communities, and families since the policy came out. Therefore, those of us who work closely on the issue do not find it surprising that there would be an increase in suicides beyond the already higher suicide rate that LGBTQ people suffer.
So we have no empirical evidence that the policy actually increased the suicide, but the anecdotal evidence and inferred evidence are extremely compelling and as such, it mustn’t be doubted that the impact of the policy will continue to be felt strongly by LGBTQ Mormons for the foreseeable future.
As problematic as the policy is, it would be wrong to place blame solely on the policy. We should address all of the factors that lead to marginalization of our LGBTQ youth, and that lead to family rejection. Focusing on the policy, but ignoring these other factors would do a disservice to the individuals we are trying to protect. Even if the policy exacerbated the problems facing LGBTQ Mormons, the primary problems have been in place for a very long time.
What immediate preventative matters can be taken?
What the research has clearly shown is that the single largest factor in teen and young adult LGBTQ people is family acceptance vs rejection. Research done by the Family Acceptance Project has clearly demonstrated this. Furthermore, it specifies what these rejecting behaviors are. Ask yourself if you think Mormon families might be doing any of the following:
- not allowing or strongly discouraging a youth from identifying themselves as LGBTQ
- not allowing their child to socialize with other LGBTQ youth
- not allowing their child to participate in supportive organizations that will help the youth cope such as a GSA
- not addressing bullying that their children face around being perceived as LGBTQ
- not protecting their child against derisive comments about LGBTQ by uninformed relatives or family friends
- engaging in derisive comments about LGBTQ people or demonizing of LGBTQ people
- not providing a family climate where a child feels safe to come out to their parents
- endorsing statements or comments that make a child fear they will be kicked out of their home or will lose their families if they come out.
These behaviors and attitudes are commonplace in Mormon families. Does anybody really doubt this? And these are some of the rejecting behaviors that raise an LGBTQ youth’s risk of suicide by 8 fold, their risk of depression by 6 fold, and their risk of drug use as well as HIV infection by 3 fold (see footnote 2).
The most effective preventions are cheap and easy. We need to educate and support parents, and we need to empower our schools to address the needs of our youth. Parents are eager and wiling to do what is best for their children. Parents need to have access to this helpful information through bishops and auxiliary leaders, through mental health providers and through school counselors. Training needs to happen. Barriers to action need to be removed.
What should the State do?
The State should take some leadership on the issue of LGBTQ youth and homeless youth. They should participate in efforts to track suicides and suicide attempts and study contributing factors. They should lift the gag rule so that LGBTQ issues can be discussed in school and should require schools to adopt anti-bullying programs that have been proven successful in other school districts. They should remove any barriers and promote the creation of GSA (Gay Straight Alliance) clubs in the school which have a proven benefit for all students (not just the LGBTQ students benefit). They should seriously address youth homelessness and invest in adequate shelters and remove legal barriers that keep agencies and outreach workers from helping these teens.
What should the Church do?
We are going to leave this up to the reader. The problem has been identified. The Church’s role in the legislative process is obvious. Their influence in the messages that go to our wards and communities about LGBTQ people is also obvious. They need to take a compassionate look at the consequences of their posture and listen to the stories of the families who have been impacted by this issue, and determine how to satisfy their theological concerns without contributing to the despair and tragedies playing out in the lives of our children.
In conclusion:
Any discussion of this issue should take into account whether we are helping or exacerbating the problem. In our opinion, this recent discussion has had an important impact by bringing much needed attention to the issue. However, sometimes the discussions have been counter-productive. As discussed above we can’t definitively know the rate of completed suicides even if the research is undertaken, so it will always be difficult to rely solely on these numbers. We also shouldn’t let our focus on one single event, such as the exclusion policy, distract us from the numerous issues that lead to distress among our LGBTQ youth and have been in place long before the policy. We need to accept that the data we have doesn’t tell us the number of suicides, but it does point to a serious problem. It also points us toward solutions. There are solutions that are effective and inexpensive.
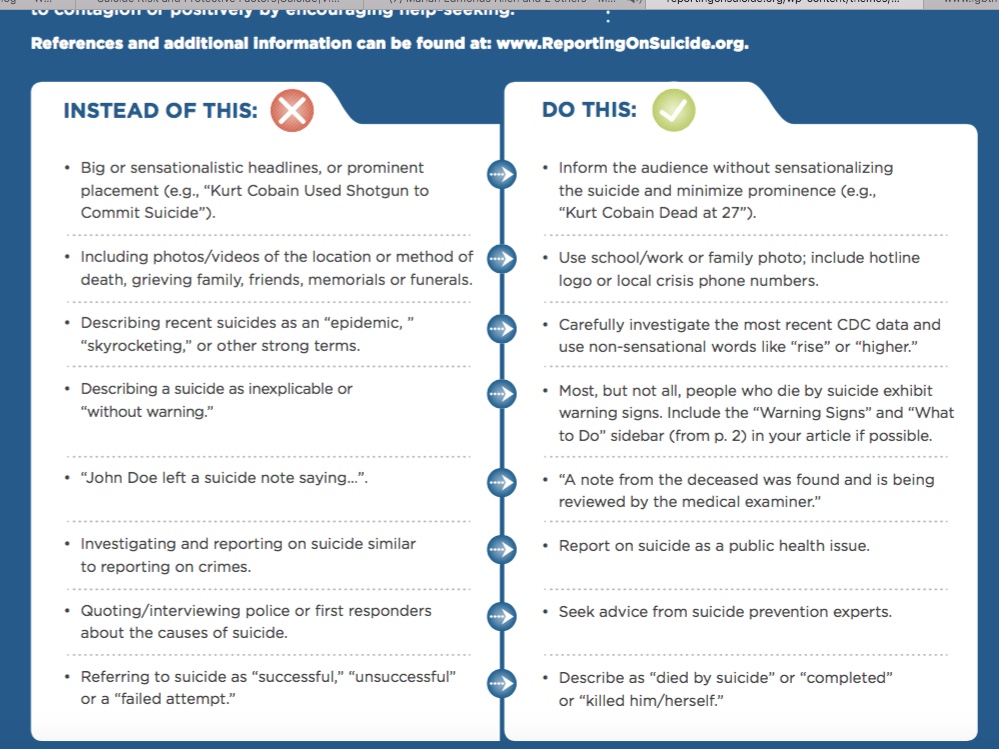
We should also be careful to follow proven guidelines about how do discuss suicide without contributing to suicide contagion. Suicide contagion or “copycat suicide” occurs when one or more suicides are reported in a way that contributes to another suicide. Suicide contagion is a real problem when suicides become high profile. We can and must discuss suicide among our youth, but we need to do it responsibly. There are proven guidelines that have been shown to avoid contagion when adopted by the media. In our new world of social media it would be responsible for each of us to familiarize ourselves with these guidelines so that we don’t unwittingly worsen the problem. Meanwhile, this discussion must continue. Avoidance will not help us address the long term issues.17
We have a public health issue: LGBTQ suicide. We don’t know how many people actually die (mortality rate), but we do know that there is a very high degree of human suffering, suicide attempts and homelessness (morbidity rate). We also have measures and tools to greatly decrease this suffering (morbidity), especially by educating parents and modifying policies (e.g eliminating gag rules around discussion of LGBTQ issues and addressing youth homelessness). We have an illness. We have a cure. Let’s implement that cure.
Resources
Please familiarize yourself with the following resources that were created to help address the problems facing our LDS LGBTQ teens:
Family Acceptance Project Please download this pamphlet that gives life-saving guidelines for families. Please share it with your Bishop and auxilary leaders. The download requires an email, but don’t let that dissuade you. They will only contact you once by this email to give a short survey and you are not required to respond. They do not share their email list.
LDSWalkWithYou.org Please familiarize yourselves with this video resource so you can share it with your friends, neighbors and ward members, especially those how might have an LGBTQ family member. These videos give the perspectives and experiences of active LDS families as they face these issues, mostly from the perspective of the parents.
Guide to talking about suicide in social media
Please be a voice for compassion in your ward. Speaking will identify you as a supporter and will require courage. And this will save lives and decrease pain. You may never find out the name of the youth who was saved because of an action you took that they witness, or that influences their family or youth leader.
Notes and Research
One of the difficulties with this post was finding the primary empirical data. As some of you may have noticed, websites, booklets, pamphlets, and blog posts will say things such as, “Studies have shown…” and then either not link to the studies or the studies can only be viewed by those who have subscriptions to the cited academic journal(s). As much as possible, Dr. Parkinson and Mike Barker wanted to provide the primary studies that have documented the problem of gay teenage suicides with small quotes from the studies. We are indebted to Dr. Mikle South, BYU Associate Professor of Psychology and Neuroscience and suicidologist – Dr. Phil Rodgers for sending many of the studies cited in this blog post. Whenever possible, the primary studies and the citations have been provided.
1 From Movement Advancement Project (LGBTmap.org) Click here to read entire PDF (click here to read entire document) Under the subheading “Research Findings on Suicide” it read in part:
“In U.S. surveys, lesbian, gay and bi adolescents and adults have two to six times higher rates of re- ported suicide attempts compared to comparable straight people. • Surveys of transgender people consistently report markedly high rates of suicide attempts.”
From the CDC (click here to read entire article):
“A nationally representative study of adolescents in grades 7–12 found that lesbian, gay, and bisexual youth were more than twice as likely to have attempted suicide as their heterosexual peers.”
The above quote from the CDC cited the following:
Russell ST, Joyner K. Adolescent Sexual Orientation and Suicide Risk: Evidence from a national study. American Journal of Public Health 2001;91:1276–1281.
Here is the abstract from Russell and Joyner’s study:
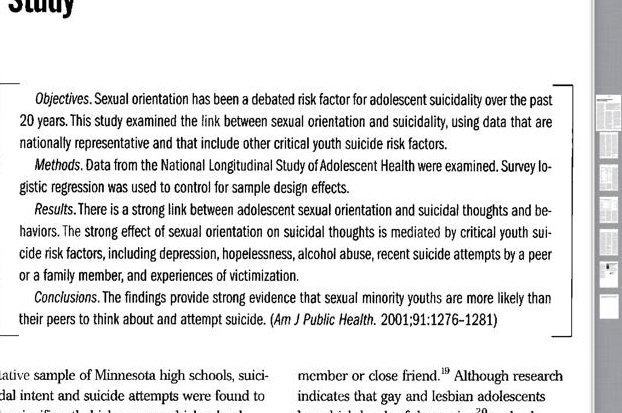
The above 2001 Russell/Joyner study, “Examined data from the National Longitudinal Study of Adolescent Health (ADD Health Study), the most recent and arguably the most comprehensive study of adolescents in the United States to date.”
Teenage suicide is usually multi-factoral and so we should use caution when oversimplifying one cause as the reason for suicide. The first page of the Russell/Joyner study states:
“Additionally, past studies have given little attention to other critical adolescent suicide risk factors. The research literature on adolescent suicide indicates that depression is a fundamental suicide risk factor for adolescents. Three other key risk factors have been well documented in past research: hopelessness, substance abuse, and the recent suicide or attempted suicide of a family member or close friend. Although research indicates that gay and lesbian adolescents have high levels of depression and substance abuse, studies of adolescent sexual orientation and suicidally, with few exceptions, have not taken these risks into account.”
The Russell/Joyner study found:
“Youths reporting same-sex sexual orientation are significantly more likely to report suicidality than their heterosexual peers. Consistent with the 1989 report of the US secretary of health and human services, our results indicate that youths with same-sex orientation are more than 2 times more likely than their same-sex peers to attempt suicide. This proportion is somewhat lower than the attempted suicide rate among youths identified as gay or lesbian in the Massachusetts study and dramatically lower than we reported in past studies of gays and lesbians from non-population-based studies.”
The CDC also cited the following 2007 study which looked specifically at transgender youth:
Grossman AH, D’Augelli AR. Transgender Youth and Life-Threatening Behaviors. Suicide & Life-Threatening Behavior 2007;37:527-537.
Here is the abstract from the Grossman/D’Augelli study:
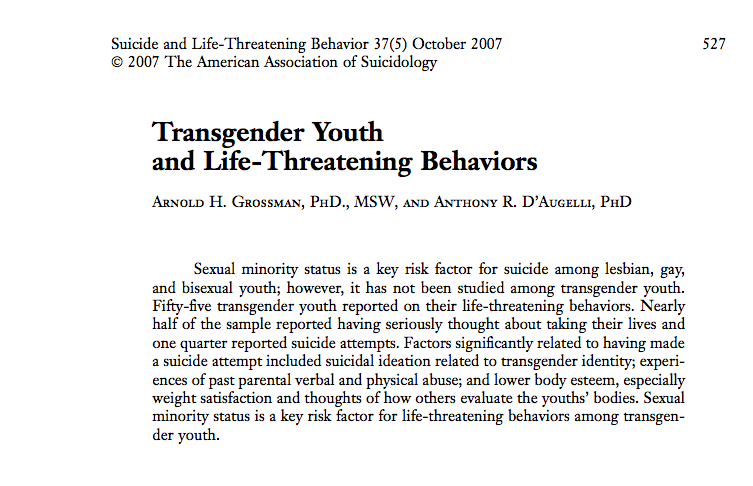
From page 532 of the study:
“Twenty-five of the transgender youth (45% of the 55 youth in the study) seriously thought about taking their lives, and 30 (55%) never had such thoughts. While 11 (20%) reported sometimes or often having seri- ous thoughts of taking their lives, 14 (26%) reported that they had rarely such thoughts…One-half of the 25 youth who seriously thought of taking their lives (n = 12) said that the thoughts were somewhat or very related to their being transgender, with more Male-to-female (MTF) youth (n = 7) than Female-to-male (FTM )youth (n = 5) relating the thoughts to their transgender identity. Of the 25 youth who ever thought seriously of tak- ing their own lives, 8 (5 MTF and 3 FTM) seriously thought of taking their lives within the last year.
“Fourteen (26%) youth reported a his- tory of life-threatening behaviors (i.e., a sui- cide attempt), 6 MTF and 8 FTM. Ten youth reported one attempt, three reported two at- tempts, and one reported 20 attempts. The ages of the youths’ suicide attempts ranged from 10 to 17; with half of the youth first attempting suicide at ages 15 or 16. All youth reporting a suicide attempt said that at least one of those attempts related to their being transgender. Ten of the 14 youth reported that the first attempt related to their gender identity. These findings were supported by their responses to the statements of transgen- der-related suicide negativity index. Six (3 each MTF and FTM) youth reported that they mainly agree or strongly agree with the statement that they tried to kill themselves because they could not accept their being transgender, while 10 (5 each MTF and FTM) of the youth gave the same responses saying that there had been times that they felt so badly about being LGBT that they wanted to be dead. Finally, 8 youth (5 MTF and 3 FTM) indicated that they mainly agree or strongly agree with the statement that they tried killing themselves because they felt that their life as an LGBT person was difficult…
“From 13% to 36% of the youth reported “sometimes” or “often” being physically abused by their parents related to their gender expression on each of the six items. More than 25% reported being slapped, beat, or hit very hard, and from 13% to 20% reported being punched, kicked, and pushed very hard. Significant differences were found between those who attempted suicide and those who did not with regard to verbal abuse and physical abuse; attempters reporting more verbal and physical abuse by their parents than non-attempters…
“The findings of this study provide evidence that transgender youth, whether MT. For FTM, are at risk for suicidal ideation and life-threatening behaviors. Almost half of the transgender youth in the study thought seri- ously of taking their lives, and half of those related these thoughts to their transgender identity. One quarter reported a suicide at- tempt, with almost three quarters of those youth relating their first or only suicide at- tempt to their transgender identity, while the remaining youth attributed subsequent at- tempts to their being transgender. This pro- portion of sexual minority youth is larger than the proportion of LGB youth found by D’Augelli et al. (2005) who attempted suicide and attributed their attempts to their sexual orientation.”
Mustanski,B, Liu R. A Longitudinal Study of Predictors of Suicide Attempts Among Lesbian, Gay, Bisexual, and Transgender Youth. Archives of Sexual Behavior (2013) 42:437–448.
Mustanksi/Liu’s abstract:
From page 438 of the Mustanksi/Liu study:
“Among studies with rigorous school-based sampling designs, all found significantly more suicidal ideation and/or attempts among LGB students than heterosexual peers (reviewed in Haas et al., 2011; McDaniel et al., 2001; Savin-Williams, 2001b). The pattern of results showing differences by sexual orientation in suicide attempts, but not deaths by suicide, may reflect the methodological limitations of performing psychological autopsy studies (King et al., 2008), a tendency to over-report attempts among LGBT youth (Savin-Williams, 2001a), or that LGBT youth may, in fact, be more likely to engage in non-lethal suicide attempt behaviors…
“Hopelessness, a common risk factor for suicidality in heterosexual youth, has also been found relevant to LGB youth(Liu&Mustanski,2012;Plo¨derl&Fartacek, 2005; Russell & Joyner, 2001; Safren & Heimberg, 1999; van Heeringen &Vincke,2000).Some research hasfound that LGB youth remain at higher risk for attempting suicide than hetero-sexual youth after controlling forsome of these general risk and protective factors (Wichstrom & Hegna, 2003), suggesting the existence of risk factors unique to LGBT youth. (emphasis mine)”
from pages 442 and 443 of the Mustanksi/Liu study:
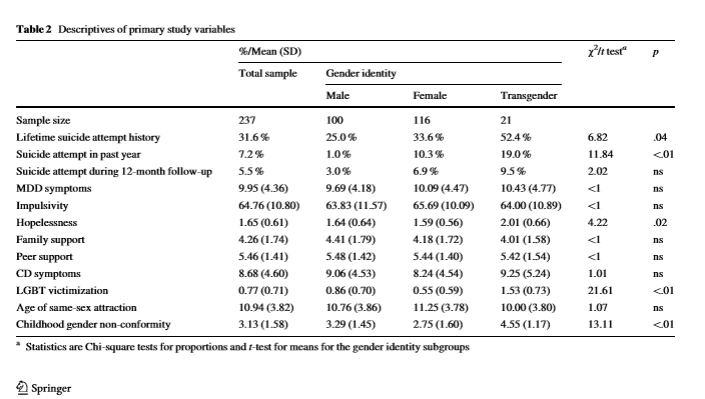
“General risk factors positively correlated with lifetime suicide attempts included Major Depressive Disorder (MDD) and Conduct Disorder (CD) symptomatology, impulsivity, and hopelessness. Among LGBT-specific risk factors, LGBT victimization was positively correlated, and age of same-sex attraction was negatively correlated, with history of attempted suicide. That is, greater experiences of LGBT victimization and younger age of same-sex attraction were associated with increased likelihood of past suicide attempts. Childhood gender non-conformity was not significantly associated with a history of suicide attempts. Among the putative protective factors included in our analyses, perceived support from family, but not peers, was negatively correlated with suicide attempt history.
“In regards to reported suicide attempts in the past year, significant positive correlations were found with MDD symptoms and hopelessness and a significant negative correlation with age of same-sex attraction. Suicide attempts during the pro-spective12-monthfollow-upperiodwerepositivelycorrelated withhopelessnessandnegativelycorrelatedwithageofsame-sexattraction.Baseline reports of lifetime and past year suicide attempts also showed medium-to-large associations with attempts during the prospective follow-up period…
“In the multivariate model with seven predictors, only depressive symptoms and hopelessness remained significantly associated with lifetime his-tory of attempted suicide. Each depressive symptom increased the odds of a lifetime suicide attempt by 17% and each unit increase in hopelessness more than doubled the odds. Effects did not meaningfully change in a model that controlled for gender, race, age, and sexual orientation. The effects of impulsivity, family support, CD symptoms, LGBT victimization, and age of first same-sex attraction had previously been significant in the bivariate analyses, but their effects were no longer significant in the multivariate model.”
From page 444 of the Mustanski/Liu study:
“Specifically, LGBT youth who attempted suicide in the past had 10 times greater odds of making another attempt during the 1-year prospective follow-up period. During the 1-year follow-up, 13 (5.5%) participants reported a suicide attempt, including 10 participants with a history of attempted suicide prior to study enrollment. Of the 75 youth who had a lifetime history of attempted suicide at baseline, 10 (13.3%) made another attempt during the 1year prospective follow-up period.”
Discussion from the Mustanski/Liu study. We decided to put it in its entirety as there is so much important information here:

2 Click here to download the free Family Education LDS Booklet from the Family Acceptance Project.
From page 438 of the previously cited Mustanksi/Liu study:
“In addition to psychiatric diagnoses, several general and LGBT-specific risk and protective factors are worth noting. One general predictor of suicide risk among adolescent sexual minorities that has emerged in several studies is social support, particularly within the family (Liu & Mustanski, 2012; Spirito & Esposito-Smythers, 2006). Hopelessness, a common risk factor.”
From page 445 of the Mustanski/Liu study:
“Additionally, we found some evidence for the role of general protective factors in lowering risk for attempted suicide. In particular, social support from parents, but not from peers, was associated with reduced risk for life time suicide attempts…
“Similarly, family-based interventions that increase support could reduce hopelessness and depression symptoms, thereby reducing the likelihood of a suicide attempt.”
From page 446 of the Mustaski/Liu study:
“Overall, our findings suggest the importance for suicide prevention programs to address both general and LGBT-specific risk factors, while also promoting social support systems available to LGBT youth, especially within families.”
3 From University of British Columbia News (UBC New). Click here to read entire article. Paragraph four reads:
“LGBTQ youth and heterosexual students in schools with anti-homophobia policies and GSAs had lower odds of discrimination, suicidal thoughts and suicide attempts, primarily when both strategies were enacted, or when the polices and GSAs had been in place for three years or more.”
4 From the Utah Department of Human Services Substance Abuse and Mental Health’s “State Suicide Prevention Programs.” Prepared October, 2015 (click here to read entire report) The First paragraph reads, in part:
“Utah has one of the highest age-adjusted suicide rates in the U.S. It was the second- leading cause of death for Utahans ages 10 to 39 years old in 2013 and the number one cause of death for youth ages 10-17. More people attempt suicide than are fatally injured.”
From page 6 of the report:
“Utah is consistently ranks above the national average for suicide deaths.”
The following data is publicly available from the Centers for Disease Control and Prevention at http://www.cdc.gov/injury/wisqars/ Chart and graphs by Dr. Phillip Rodgers, Ph.D
Note: While Utah suicide rates are higher than the National average, they are generally in line with other Rocky Mountain States
Note: Suicide is a complex behavior that is influence by multiple factors that vary across individuals.


5 In a study by Mark Hatzenbuehler of Columbia University found that homosexual teen suicide rates were raised in unsupportive environments (click here to read article).
“The results of this study are pretty compelling,” Hatzenbuehler said in a statement. “When communities support their gay young people, and schools adopt anti-bullying and anti-discrimination policies that specifically protect lesbian, gay, and bisexual youth, the risk of attempted suicide by all young people drops, especially for LGB youth.”
6 Rosenstreich G. LGBTI People: Mental Health & Suicide. Briefing Paper, Revised 2nd Edition, 2013 (click here to read entire paper). The cited statistic is taken from page 7 of the paper.
7 see STRIB op-ed by Dr. Mikle South, Feb 7, 2016 (click here to read article).
“Some may not realize that Utah belongs to the so-called “suicide belt” along the Intermountain Corridor. Suicide rates throughout this region are considerably higher than anywhere else in the country save Alaska, where rates are more than double the national average.”
7a CDC (click here to read)
8 Hatzenbuehler ML, Ballatorre A, Lee Y, Finch B, Muennig P, Fiscella K. Structural Stigma and All-Cause Mortality in Sexual Minority Populations. Social Science & Medicine 2013 Feb; 103: 33-41 (click here to read entire study)
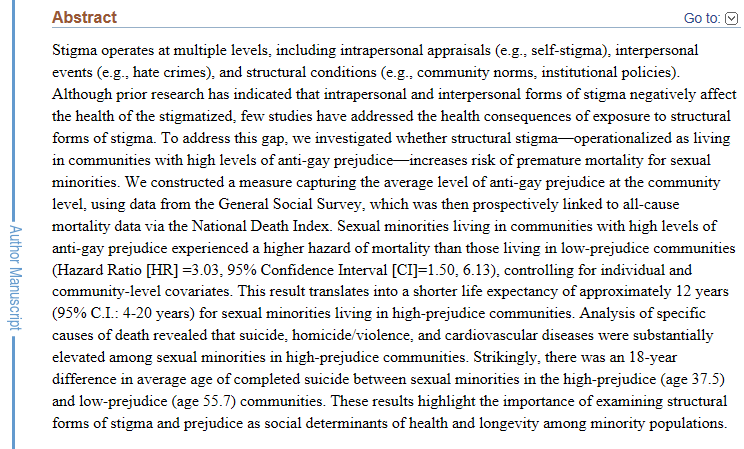
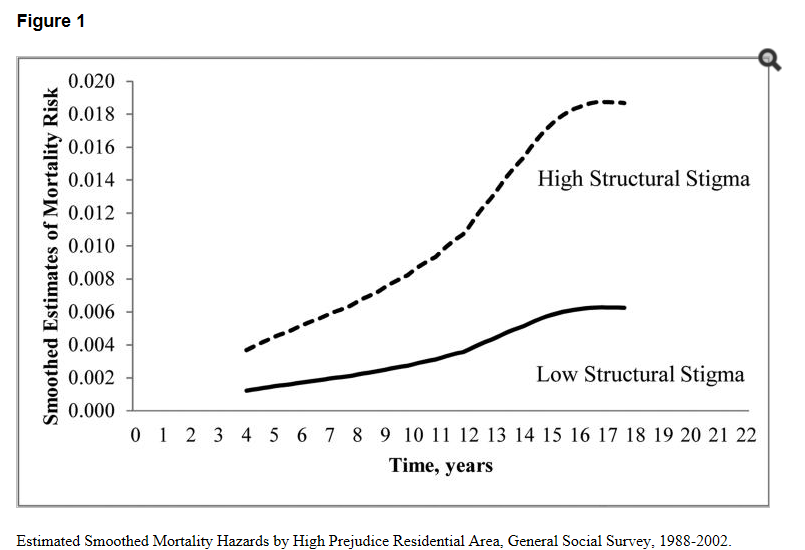
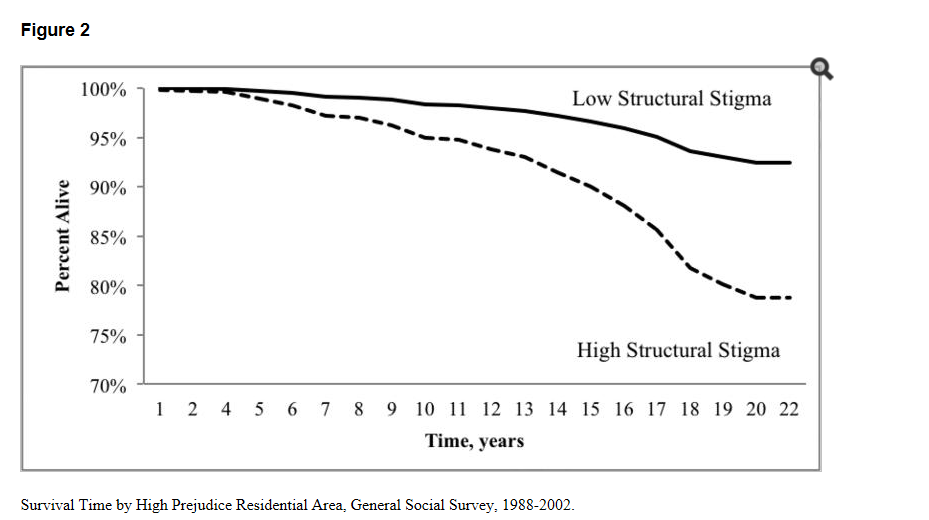
First part of the study’s Discussion. Again, if you would like to read the entire study, click on the link at the beginning of footnote 6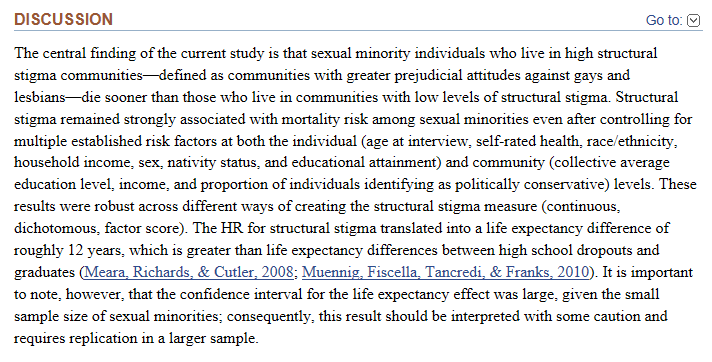
This study was cited in a February U.S. New and World Report article in which one of the study’s researchers, Mark Hatzenbuehler stated (click here to read entire article):
“The results from the current study provide important social science evidence demonstrating that sexual minorities living in communities with high levels of anti-gay prejudice have increased risk of mortality, compared to those living in low-prejudice communities.”
Meanwhile, there is actually evidence that homosexuals are not at any increased risk of mental illness when they are in a less homophobic community. A study published in the journal Psychosomatic Medicine, by researchers at the University of Montreal (lead author Robert-Paul Juster), shows that, “as a group, gay and bisexual men who are out of the closet were less likely to be depressed than heterosexual men and had less physiological problems than heterosexual men.” (click here to read a U.S. News and World Report article about this study). It is relevant that the subjects of this study live in Montreal which is considered one of the least homophobic cities in North America (evidenced in part by Quebec being the first government in the world to recognize same-sex civil unions, even before Netherlands).
A Concordia University doctoral thesis in clinical psychology investigated and examined environmental risks and protective factors that counterbalance the severe mental illnesses that LGB youth have and the role of cortisol, which is a hormone that is released in situations of stress leading to physical and mental health consequences.
“Compared to their heterosexual peers, suicide rates are up to 14 times higher among lesbian, gay and bisexual high school and college students,” says Michael Benibgui, who led this investigation as part of his PhD thesis at Concordia’s Department of Psychology and Centre for Research in Human Development…
“Benibgui says abnormal cortisol activity in LGB youth, combined with the vicious cycle of stress, could be further influenced by a complex set of biological, psychological and social factors. “This study shows a clear relation between abnormal cortisol levels and environmental stressors related to homophobia,” (click here to read more).
8a National Conference of State Legislatures (NCSL) October 1, 2013 (click here to read more).
“Between 20 and 40 percent of homeless youth identify as Gay, Lesbian, Bisexual, Transgender or Questioning (GLBTQ)”
Peggy Fletcher Stack, “Program Aims to Stop Suicide, Homelessness in LGBT Mormon Youth,” Salt Lake Tribune, March 15, 2014. Click here to read entire article. The article reads in part:
“More than 5,000 youth are estimated to experience homelessness in Utah per year. Of these, at least 40 percent are LGBT and the majority are from religious and socially conservative families, with 60 percent from Mormon homes.”
9 From a study in the March 1, 2001 issue of the American Journal of Epidemiology, which targeted Utah men between the ages of 15 and 34, and cross-referenced their activity in the Church of Jesus Christ (click here to read more). This was previously cited in footnote 5
From the abstract:
“Although the mechanism of the association is unclear, higher levels of religiosity appear to be inversely associated with suicide.”
From the discussion:
“we suggest that even if the mechanism of the association is not understood between religiosity and suicide, low religiosity is an attribute that could be used to identify a group that has an increased risk of suicide. Insofar that risk and protective factors for suicide are identified and quantified, public health efforts to reduce suicide have an increased likelihood of being effective.”
This is sobering if you also take into account that LGBTQ people overwhelmingly leave the church or are kicked out. (see Dehlin study cited below). This is not surprising since loss of community/close social relationship is a known factor in suicide.
Take the above findings in light of the following study which looked at 1,612 Mormons and former-Mormons who engaged in sexual orientation change efforts (SOCE):
Dehlin JP, Galliher RV, Bradshaw WS, Hyde DC, Crowell KA. Sexual Orientation Change Efforts Among Current or Former LDS Church Members. Journal of Counseling Psychology March 2014; 62(2). (click here to read entire study)
From the abstract:
“Data were obtained through a comprehensive online survey from both quantitative items and open-ended written responses. A minimum of 73% of men and 43% of women in this sample attempted sexual orientation change, usually through multiple methods and across many years (on average).”
From this data we can probably assume that most LGBTQ Mormons have engaged in SOCE
page 3, under the heading “Participants”
“Regarding LDS church affiliation, participants described themselves as follows: 28.8% as active (i.e., attending the LDS church at least once per month), 36.3% as inactive (i.e., attending the LDS church less than once per month), 25.2% as having resigned their LDS church membership, 6.7% as having been excommunicated from the LDS church, and 3.0% as having been disfellowshipped (i.e., placed on probationary status) from the LDS church
From this data we can assume that most LGBTQ Mormons end up leaving the LDS Church
page 8, under heading “The Nature of SOCE”
“Highly religious LDS men unsupportive families and communities were most likely to report having engaged in SOCE, while LDS women were somewhat less likely to do so. These findings confirm previous research that SOCE efforts most often arise from religious and/or social pressure (APA, 2009). The finding that same-sex-attracted LDS women were less likely to engage in SOCE seems noteworthy, though the exact reasons for this are still unknown. Same-sex attracted LDS women may feel less pressure to engage in SOCE because of the greater sexual fluidity afforded women within the constraints of socialized gender roles (Diamond, 2009); U.S. male culture tends to stigmatize male homosexuality more than female homosexuality or bisexuality (Herek, 2002). The role of LDS cultural factors, such as the church’s historical emphasis on missionary service for 19-year-old men with an accompanying requirement for sexual worthiness also warrants investigation.”
Adding this to the above data points, can we make the following inferences -that, most highly-religious LGBTQ LDS men have attempted SOCE, have families who are unsupportive (thus removing one protection against suicide attempts), and end up leaving the LDS Church (removing another protective barrier against suicide attempts).
10 This footnote cites three studies. The most recent one is from 2015
Jeremy J. Gibbs & Jeremy Goldbach (2015) Religious Conflict, Sexual Identity,and Suicidal Behaviors among LGBT Young Adults, Archives of Suicide Research, 19:4, 472-488, DOI: 10.1080/13811118.2015.1004476 (to access the study click here)
from the Discussion of the Gibbs/Golbach study (page 483)
“After consideration of internalized homophobia, the relationship between leaving one’s religion and suicidal thoughts was significant. In our analysis, leaving one’s religion is associated with a decrease in internalized homophobia. However, while this expected relationship emerged, we also found that leaving one’s religion was associated with a higher risk of suicidal thoughts. Thus, a dual relationship was found where leaving the religion was related to lower internalized homophobia, leading to lower odds of suicidal thoughts, but also an increase in the odds of suicidal thoughts directly. Further, the strength of the direct effect and indirect effect suggests that leaving one’s religion of origin has a sum impact of increasing the odds of suicidal thoughts, a potentially important clinical implication for those working with LGBT persons who are struggling to come to terms with both religious and LGBT identities. As our measure was an indicator of conflict, it is possible it was also measuring an addition construct (e.g., those who leave their religion may experience a disruption in their support system). This indicator, as well as parental anti-homosexual religious beliefs, may be measuring both conflict and problems in primary support. Concerns with our current measurement of minority stress constructs have been noted in other literature (Goldbach, Tanner-Smith, Bagwell et al., 2013).
Internalized homophobia was not associated with suicide attempt in the last year. Conversely, parental beliefs and leaving the religion of origin were associated with a suicide attempt in the last year. This has important implications on clinical practice, as direct interventions that are focused on reducing suicide by diminishing feelings of internalized homophobia alone may be ineffective with this population. Further, this finding suggests that relationships (parental, and religious community) may have more impact on deterring a suicide attempt than one’s own gay self-concept, and adds evidence for family-centered approaches such as those being explored by other researchers in the area (e.g., Family Acceptance Project; Ryan, Russell, Huebner et al., 2010)..
“There were two important clinical implications found in the current study. First, it may seem counterintuitive that when individuals choose to leave their religion in order to experience more self acceptance that they inadvertently experience more risk for suicide. Clinicians should be aware that leaving one’s religion of origin may add additional stressors that ultimately place a client at additional risk for suicide. Further, the negative impact felt from leaving one’s religion due to conflict has a stronger impact than the positive indirect impact through a reduction in internalized homophobia. As many LGBT young adults often experience multiple levels of loss, clinical interventions should ideally entail a plan for enhancing supportive resources without risk of further isolation from communities of historical significance to the client (i.e., loss of community, potential loss of protective belief structure). This may involve encouraging clients to be involved in communities that incorporate their religious tradition and their LGBT identity, which has been found qualitatively to be supportive (Jaspal & Cinnerella, 2010; Thumma, 1991). Second, it is apparent that LGBT young adults who experience religious identity conflict are at significant risk for suicide. When individuals experience conflict with an accepted belief structure this can cause a great deal of distress, which may lead to a desire to escape. For this reason, suicide risk assessments could be enhanced by further understanding the loss of spiritual resources and subsequent challenges adjusting to this loss.”“In our study, those who experienced a religious upbringing and are currently experiencing religious conflict were most at risk of considering suicide. Further, a religious upbringing in itself does not provide protection from suicidal ideation when compared to a non-religious upbringing. Thus, it appears that a religious upbringing that includes unresolved religious and LGBT identity conflict puts an individual more at risk of suicidal thoughts.
Kralovek K, Fartacek C, Fartacek R, Ploderl M. Religion and Suicide Risk in Lesbian, Gay and Bisexual Austrians. Journal of Religion and Health. 2014; 53:413-423
To see how religion and suicide in Utah intersect, see the following study:
Hilton SC, Fellingham GW, Lyon JL. Suicide Rates and Religious Commitment in Young Adult Males in Utah, American Journal of Epidemiology March 2001; volume 155 issue 5; pages 413-419 (click here to read study)
From the Hilton/Fellingham abstract:
“Although the mechanism of the association is unclear, higher levels of religiosity appear to be inversely associated with suicide.”
From the discussion:
“we suggest that even if the mechanism of the association is not understood between religiosity and suicide, low religiosity is an attribute that could be used to identify a group that has an increased risk of suicide. Insofar that risk and protective factors for suicide are identified and quantified, public health efforts to reduce suicide have an increased likelihood of being effective.”
Here is the abstract from the Hilton/Fellingham study:
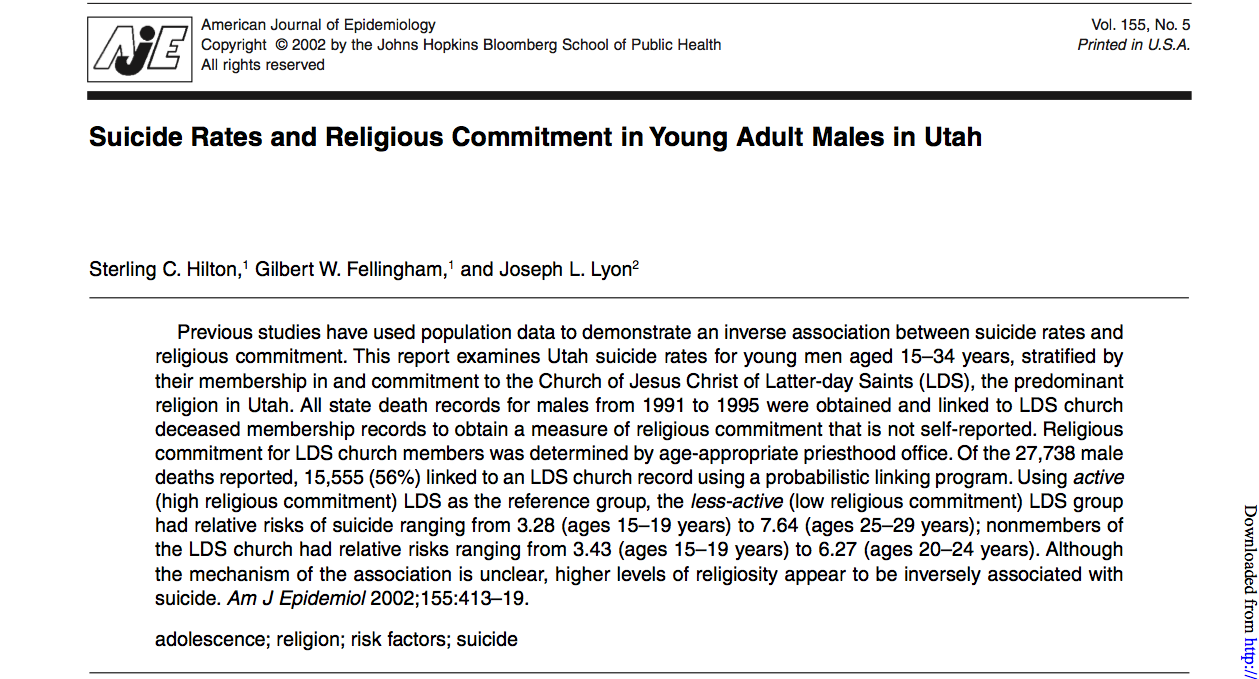
Table from the study:
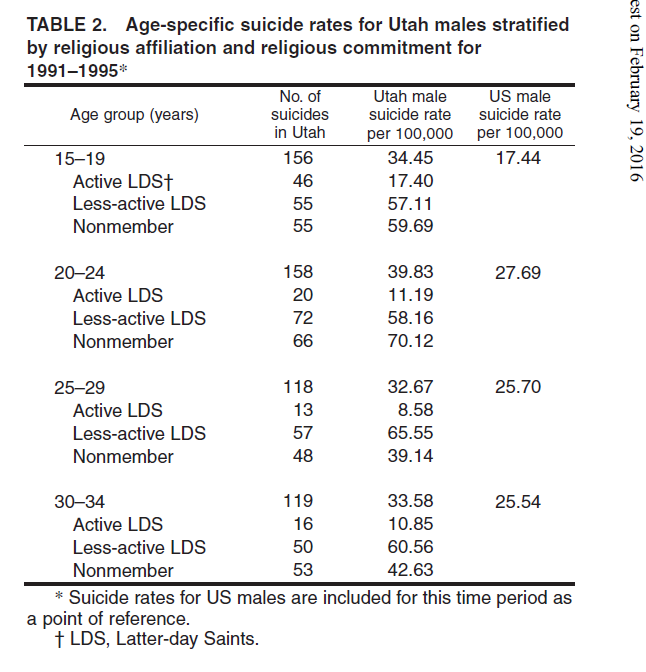
Table 3 from the study:
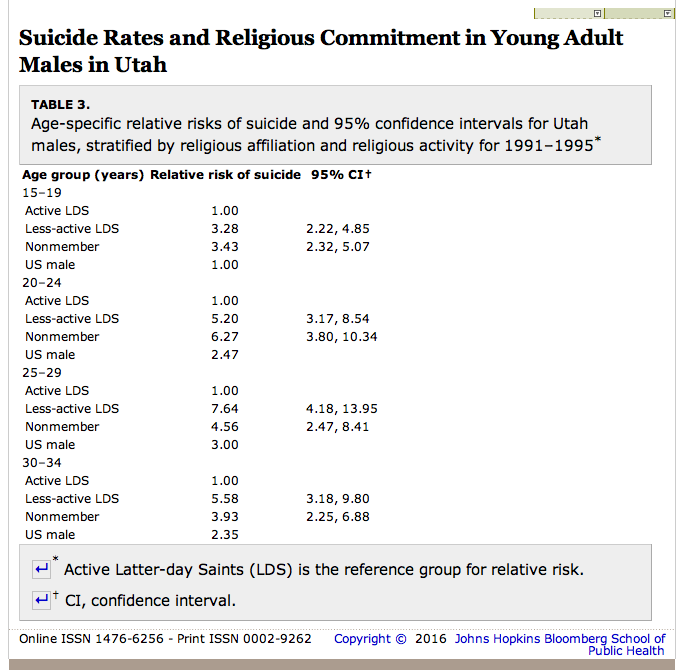
Results:
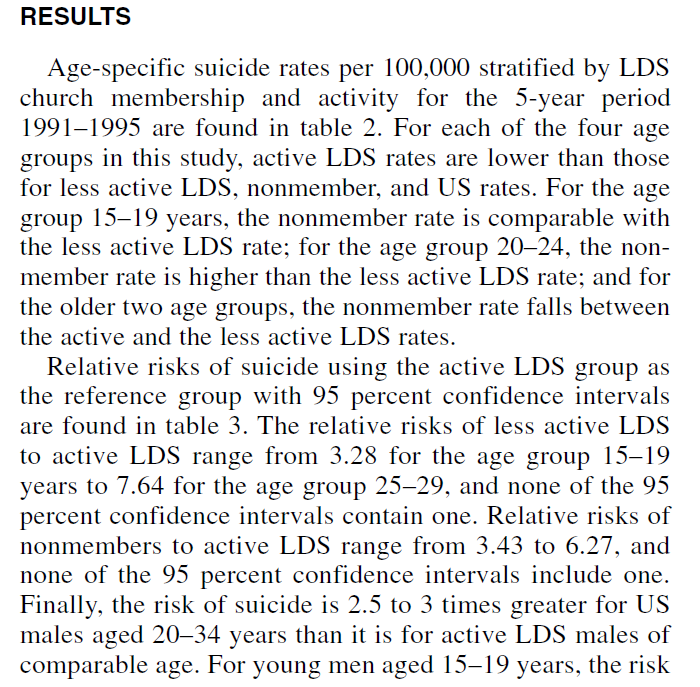
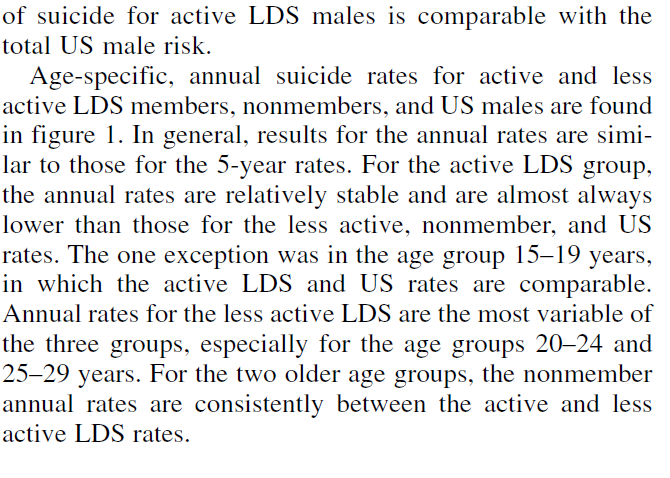
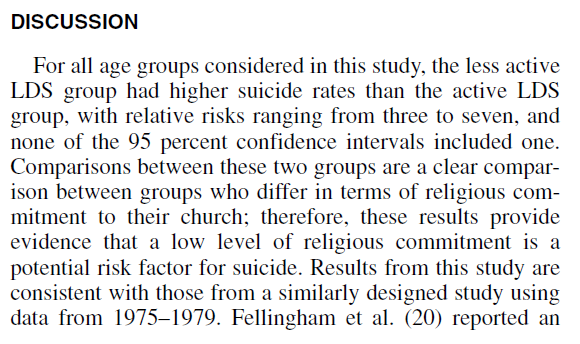
From the Discussion:
“For all age groups considered in this study, the less active LDS group had higher suicide rates than the active LDS group…”
11 Peggy Fletcher Stack, “Suicide Fears, If Not Actual Suicides, Rise in Wake of Mormon Same-Sex Policy,” Salt Lake Tribune, January 28, 2016. Click here to read the article in its entirety. Part of the article reads:
“From the policy’s onset through the end of 2015, Montgomery, a leader of the Mama Dragons support group for the families of gay Latter-day Saints, says she had counted 26 suicides of young LGBT Mormons in Utah — 23 males, one female and two transgender individuals — between ages 14 and 20.
She tallied another six in other states — though none of the reported deaths could be specifically tied to the policy…
Trouble is, the number far exceeds the suicide figures collected by the Utah Department of Health.
Preliminary figures for November and December show 10 suicides in the Beehive State for people ages 14 to 20, with two more cases “undetermined.”
In fact, the department reports, the overall number of Utah deaths for that age group in those months was 25, including the 10 suicides and two “undetermined” cases, along with 11 in accidents, one by natural causes and one homicide.
“We monitor the numbers [of youth suicides] very closely. We review them every month,” says Teresa Brechlin, who works in the department’s violence- and injury-prevention program. “If we had seen such a huge spike, we would have been investigating it.”
Had there been any mention of the LDS Church’s policy on gays, her department “would have noted that,” Brechlin adds. “We have not seen that at all.”
12 Mike Barker has asked a suicidologist, several LGBTQ advocates, two forensic specialists,(none of these people questioned are from Utah) and at least one Utah law maker who is concerned about gay teen suicide, if there are aware of any states, that as part of the suicide investigation, perform what is called a “psychological autopsy” with regards to the deceased’s sexuality. The answer has been no.
13 Ann P. Haas PhD, Mickey Eliason PhD, Vickie M. Mays Ph,MSPH, Robin M. Mathy MAMSWMStMSc, Susan D. Cochran PhDMS, Anthony R. D’Augelli PhD, Morton M. Silverman MD,Prudence W. Fisher PhD, Tonda Hughes PhDRNFAAN, Margaret Rosario PhD, Stephen T. Russell PhD, Effie Malley MPA, Jerry Reed PhDMSW, David A. Litts OD, Ellen Haller MD, Randall L. Sell ScD, Gary Remafedi MDMPH, Judith Bradford PhD, Annette L. Beautrais PhD, Gregory K. Brown PhD, Gary M. Diamond PhD, Mark S. Friedman PhDMSWMPA, Robert Garofalo MDMPH, Mason S. Turner MD, Amber Hollibaugh & Paula J. Clayton MD (2010): Suicide and Suicide Risk in Lesbian, Gay, Bisexual, andTransgender Populations: Review and Recommendations, Journal of Homosexuality, 58:1, 10-51 (to read the study in its entirety, click here)
Under the subtitle of the Haas study, “SUICIDE AND SUICIDE ATTEMPTS IN LGB POPULATIONS” we read:
“Because death records do not routinely include the deceased person’s sexual orientation, there is no official or generally reliable way to determine rates of completed suicide in LGB people. Some researchers have attempted to determine whether these groups are overrepresented among those who die by suicide, using “psychological autopsy” reports of family and friends to determine the decedents’ sexual orientation. Several studies using this method have been published, focusing on young adult male suicides in San Diego (Rich, Fowler, Young, & Blenkush, 1986) and adolescent suicides in the New York metropolitan area (Shaffer, Fisher, Hicks, Parides, & Gould, 1995) and the province of Quebec (Renaud, Berlim, Begolli, McGirr, & Turecki, 2010). Each of these studies has concluded that same-sex sexual orientation is not disproportionately represented among suicide victims.
“To date, psychological autopsy studies that have examined sexual orientation have used relatively small samples and have identified very few suicide decedents as having minority sexual orientation. In the New York study, 3 of 120 adolescent suicide decedents and none of a similar number of living community control subjects with whom the suicide victims were compared, were found to have a same-sex orientation (Shaffer et al., 1995). The Quebec study similarly identified same-sex orientation in 4 of 55 suicide adolescent suicide victims and none of the community control subjects (Renaud et al., 2010). Minority sexual orientation may have been underreported by key informants in these studies because they were not aware of, or chose to withhold this information (Renaud et al., 2010). In any case, conclusions based on the small numbers reported must be regarded as tentative.
“The San Diego study lacked a living control group and has been criticized based on the researchers’ assumption that the 11% of young male suicide decedents who were identified as gay approximated the expected prevalence rate for young gay men in the population under study (McDaniel, Purcell, & D’Augelli, 2001). Using a more likely prevalence rate of 3–4% would have suggested that young gay men were overrepresented among suicide decedents by a factor of at least three.
“Recent studies have used Denmark’s extensive registries of vital statistics and other sociodemographic data to examine whether people in same-sex registered domestic partnerships (a proxy indicator of sexual orientation) were overrepresented among suicide decedents. The Danish data can be matched fairly easily because individual information recorded in the various registries uses unique identification numbers assigned to citizens at birth. One study that linked Danish mortality and sociodemographic data (Qin, Agerbo, & Mortensen, 2003) noted that same-sex registered domestic partners were 3–4 times more likely than heterosexual married persons to die by suicide, although this was not a key focus of the study and corroborating data were not presented. A subsequent study that was designed explicitly to examine suicide risk in Denmark by sex and relationship status (Mathy, Cochran, Olsen, & Mays, 2009) found that elevated risk of suicide in same-sex partnered people was concentrated almost exclusively among men. Men who were currently or formerly in same-sex domestic partnerships were eight times more likely to die by suicide compared to men with histories of heterosexual marriage, and almost twice as likely as men who had never married. Although small numbers of cases limited the precision of the analyses, same-sex partnered men appeared to have an elevated risk of suicide across the lifespan. Women in current or former same-sex domestic partnerships did not show significantly higher risk of suicide mortality compared to hetero-sexually married or never-married women. A limitation of the approach used in the Danish studies is that it captures suicide deaths only among partnered and officially registered LGB people. Further, opportunities for replication in other countries have been limited, but these may expand as more as more countries and U.S. states officially recognize and record same-sex marriages and partnerships (Strohm, Seltzer, Cochran & Mays, 2009).
“An 18-year follow-up study of the mortality status of over 5,000 U.S. men aged 17–59 who were interviewed in the Third National Health and Nutrition Examination Survey (1988–1994) found no suicide deaths among the 85 men who reported having any lifetime same-sex sexual partner (Cochran & Mays, 2011). Findings from this study, in stark contradiction to the Danish registry studies, suggest that suicide mortality may not be elevated among U.S. men who have sex with men. The authors cautioned, however, that the number of men who reported same-sex sexual behavior in this survey was quite small, and that elevated risk of suicide mortality among U.S. men may yet be observed in studies with larger samples and a longer follow-up period.”
This needs some explaining.
This paper points out some confusing and seemingly contradictory results from a handful of studies with small sample sizes and it highlights the problems that come when trying to determine the causes of suicides. Suicide attempts are much easier to study, because you can talk to the victim and get a first hand report of factors that played a role. As of now, a suicide attempt is not always a strong predictor of completed suicide e.g. four out of five people (80%) who die by suicide are male. However, three out of every four people (75%) who make a suicide attempt are female (LGBTmap.org).
With suicide deaths, all you can get is limited information from families and other informants who may be unaware of the victims sexual orientation, or may be unwilling to discuss it for any number of reasons. Some of these studies could not confirm a higher rate of suicide among LGBTQ people. Others suggest there might be. At this point, the data that would tell us if LGBTQ people are at higher risk for death by suicide is simply not available.
Meanwhile, our public health response should be based on morbidity AND mortality. Elevated risk of suicide attempts is cause enough to respond, because it is a reflection of morbidity; it is a reflection of human suffering and disability that has a solution. In fact many communities in our country have already implemented the solutions and have seen good results. Whatever the rate of suicide deaths, that number can and will drop if we address the causes of despair and isolation that drive the suicide attempts. Lowering suicide attempts will lower completed suicides.
13a A Tale of Two Mormons, Feast of Fun podcast, episode 2279, January 27, 2016 (click here to listen)
13b President Marion G. Romney, “We Believe in Being Chaste,” September 1981 Ensign (click here to read)
“Some years ago the First Presidency said to the youth of the Church that a person would be better dead clean than alive unclean.
“I remember how my father impressed the seriousness of unchastity upon my mind. He and I were standing in the railroad station at Rexburg, Idaho, in the early morning of 12 November 1920. We heard the train whistle. In three minutes I would be on my way to Australia to fill a mission. In that short interval my father said to me, among other things, “My son, you are going a long way from home. Your mother and I, and your brothers and sisters, will be with you constantly in our thoughts and prayers; we shall rejoice with you in your successes, and we shall sorrow with you in your disappointments. When you are released and return, we shall be glad to greet you and welcome you back into the family circle. But remember this, my son: we would rather come to this station and take your body off the train in a casket than to have you come home unclean, having lost your virtue.”
Elder Boyd K. Packer, “Message to Young Men,” Priesthood Session, October 1976 General Conference. Every talk from the October 1976 General Conference has a written transcript available on LDS.org, except this talk by Elder Packer. We wonder why? To listen to his talk, click here. To read the written transcript, click here. The following is part of Elder Packer’s talk. Perhaps this is the reason the written transcript is no longer available on LDS.org:
“It was intended that we use this power only with our partner in marriage. I repeat, very plainly, physical mischief with another man is forbidden. It is forbidden by the Lord.
There are some men who entice young men to join them in these immoral acts. If you are ever approached to participate in anything like that, it is time to vigorously resist.
While I was in a mission on one occasion, a missionary said he had something to confess. I was very worried because he just could not get himself to tell me what he had done.
After patient encouragement he finally blurted out, “I hit my companion.”
“Oh, is that all,” I said in great relief.
“But I floored him,” he said.
After learning a little more, my response was “Well, thanks. Somebody had to do it, and it wouldn’t be well for a General Authority to solve the problem that way”
I am not recommending that course to you, but I am not omitting it. You must protect yourself.”
14 Rev. Marian Edmonds-Allen, “Suicides or Not, LDS Is Harming LGBT Youth,” Advocate, February 3, 2016. Click here to read entire article.
15 Click here to read the Utah code. It reads:
Effective 5/13/2014
53A-13-302. Activities prohibited without prior written consent — Validity of consent — Qualifications — Training on implementation.(1) Except as provided in Subsection (7), Section 53A-11a-203, and Section 53A-15-1301, policies adopted by a school district or charter school under Section 53A-13-301 shall include prohibitions on the administration to a student of any psychological or psychiatric examination, test, or treatment, or any survey, analysis, or evaluation without the prior written consent of the student’s parent or legal guardian, in which the purpose or evident intended effect is to cause the student to reveal information, whether the information is personally identifiable or not, concerning the student’s or any family member’s:
(a) political affiliations or, except as provided under Section 53A-13-101.1 or rules of the State Board of Education, political philosophies;(b) mental or psychological problems;
(c) sexual behavior, orientation, or attitudes;
(d) illegal, anti-social, self-incriminating, or demeaning behavior;
(e) critical appraisals of individuals with whom the student or family member has close family relationships;
(f) religious affiliations or beliefs;
(g) legally recognized privileged and analogous relationships, such as those with lawyers, medical personnel, or ministers; and
(h) income, except as required by law.
Also see October 22, 2015 article in the Utah Political Capitol (click here to read). It reads in part:
“However, the law is quite clear. Dabakis is referring to 53(A)-13-302(1) of Utah Code that states that “Policies adopted by a school district or charter school…shall include prohibitions on the administration to a student of any psychological or psychiatric examination, test, or treatment, or any survey, analysis, or evaluation without the prior written consent of the student’s parent or legal guardian, in which the purpose or evident intended effect is to cause the student to reveal information…concerning the student’s or any family member’s…sexual behavior, orientation, or attitudes.”
“In short, administrators are stuck in a legal Catch 22 – If a student reports that they are suicidal, administrators are required to tell parents of this fact – but telling a parent that as child suicidal, and therefore providing an evaluation, because they feel rejected for their sexual orientation is also illegal. An administrator may know, but they are legally prevented from taking action.”
16 There are exceptions, such as the underutilized website, gaysandmormons.org, and Elder Oaks’ October 2012 General Conference address entitled, “Protect the Children,” in which he stated:
“Young people struggling with any exceptional condition, including same-gender attraction, are particularly vulnerable and need loving understanding—not bullying or ostracism.” (click here to read entire talk)
17 See reportingonsuicide.org and lgbtmap.org
Sincere appreciation to the following people for giving us resources, information and insights on this issue so that we were able to pull together this information:
-Dr. Phil Rogers
-Dr Mikle South
-Rev. Marian Edmonds-Allen
-Kendall Wilcox
-Thomas Montgomery
-Wendy Montgomery
-Lori Burkman
Dr. Daniel Parkinson and Michael Barker, PA-C
DR. DANIEL PARKINSON was born and raised in Utah to a Mormon family with a thick Mormon Heritage. He comes to this issue as a psychiatrist, with a strong sense of activism, and a desire to help the two communities that he inherited as his birthright: the Mormon community, and the gay community. He administrates the GayMormonStories.org podcast and the NoMoreStrangers.org blog. MICHAEL BARKER, PA-C is one of the proprietors of the Rational Faiths blog and works as a Physician Assistant in Southern Oregon
All posts by Dr. Daniel Parkinson and Michael Barker, PA-C



This is such an important post! Thank you for all the effort that went into it.
Just an FYI! The VOA Homeless Resouce Center is opening a larger shelter for ages 22 and under at the end of May 2016!! There will be more beds, case managers, free law clinic, among other things.
The church should seriously look at this article, acknowledge how it fosters a bad environment for LGBTQ youth, and then make the necessary policy changes to make things better for the affected youth. In other words the church needs to admit its role in this and change its policies. A great place to start would be letting the members know it is sin to from shun or kick their children out of the house for being born LGTBQ. The homelessness problem needs to immediately stop.
Daniel and Michael. I deeply appreciate the professional and logical layout of this post. I am sure it took quite some time to make and I will certainly be pointing others to it.
Thank you, Dr. Daniel Parkinson and Michael Barker, PA-C.
While reading through this, I couldn't shake the feeling of absurdity. Maybe it's because this got me thinking about my Grandkids and I imagined them growing to be their best self only to be convinced, by a church, they are an abomination. Reading through data of child suicide spikes and their possible correlation with Mormon exclusionary doctrine, feels unreal. It's a sober idea that, before we speak out too strongly, we need to be sure that Mormon youth aren't just killing themselves at the regular same old elevated rate. Growing up Mormon, I heard so many times, "By their fruits ye shall know them". What a self-damning statement.
Religion at its best, helps calm our fears surrounding death and promotes the Golden Rule. Why have we let it become instead, it's worst self, the harmful cynic. How have we given this cynic access to the hearts of our children who are born different. What God creates a meandering stream and commands it to be a straight ditch?
Thank you for doing the enormous amount of work to create this important resource. My frustration is how to share it with active Mormons. When I mentioned to my kind, loving, former bishop brother that way too many GLBTQ Mormon young people have committed suicide, he just said. “I hope not!”
Lori Burkman,
And thanks for editing it!!!
Jessica,
Thanks for giving us a heads-up.
Exiled,
Daniel and I agree with you a million percent.
A Happy Hubby,
Thanks for reading it. It was super long for a blog-post, but Daniel and I didn’t want to short-change anyone with this important information.
Jeremy Gibbons,
That was beautiful what you wrote.
Marilyn Johnson,
I have LDS colleagues with whom I have shared part of these statistics. Some have said, “Oh. That’s too bad.” And I’m thinking, “Ya!!!! So what are you going to do about it?”
Jerilyn Pool is reformatting the post into a PDF format that will be available at the blog to print for the use by bishops, stake presidents, and run-of-the-mill members. So it’s coming.
Also, Dr. Boyd Jay Peterson has approached Daniel and me about reworking this post so it can be published in Dialogue: A Journal of Mormon Thought. This way it won’t be lost in the belly of the internet.
A Happy Hubby,
I forgot to mention that Jerilyn Pool is reformatting this blog-post into a PDF so it will be available to print and hand out.
“The data reported by Wendy Montgomery seem confusing because, while she did get a high number of reports of suicide since November 6, it is hard to square these numbers with the State of Utah who reports that there were only 10 suicides in Utah in November and December of 2015 in the 14-20 age range. ”
How is this hard to square. You do realize that there are LDS people outside Utah right? And that these reports could be coming in from other areas?